
Clinical AI often fails to earn clinician trust because it silently degrades, floods staff with false alarms, and hides uncertainty. This article examines the root causes—silent and reasoning drift, poor UI design, and lack of feedback loops—and outlines concrete engineering practices such as safety shells, calibrated uncertainty displays, structured override capture, and trust‑centric monitoring metrics to turn skeptical doctors into collaborative partners.
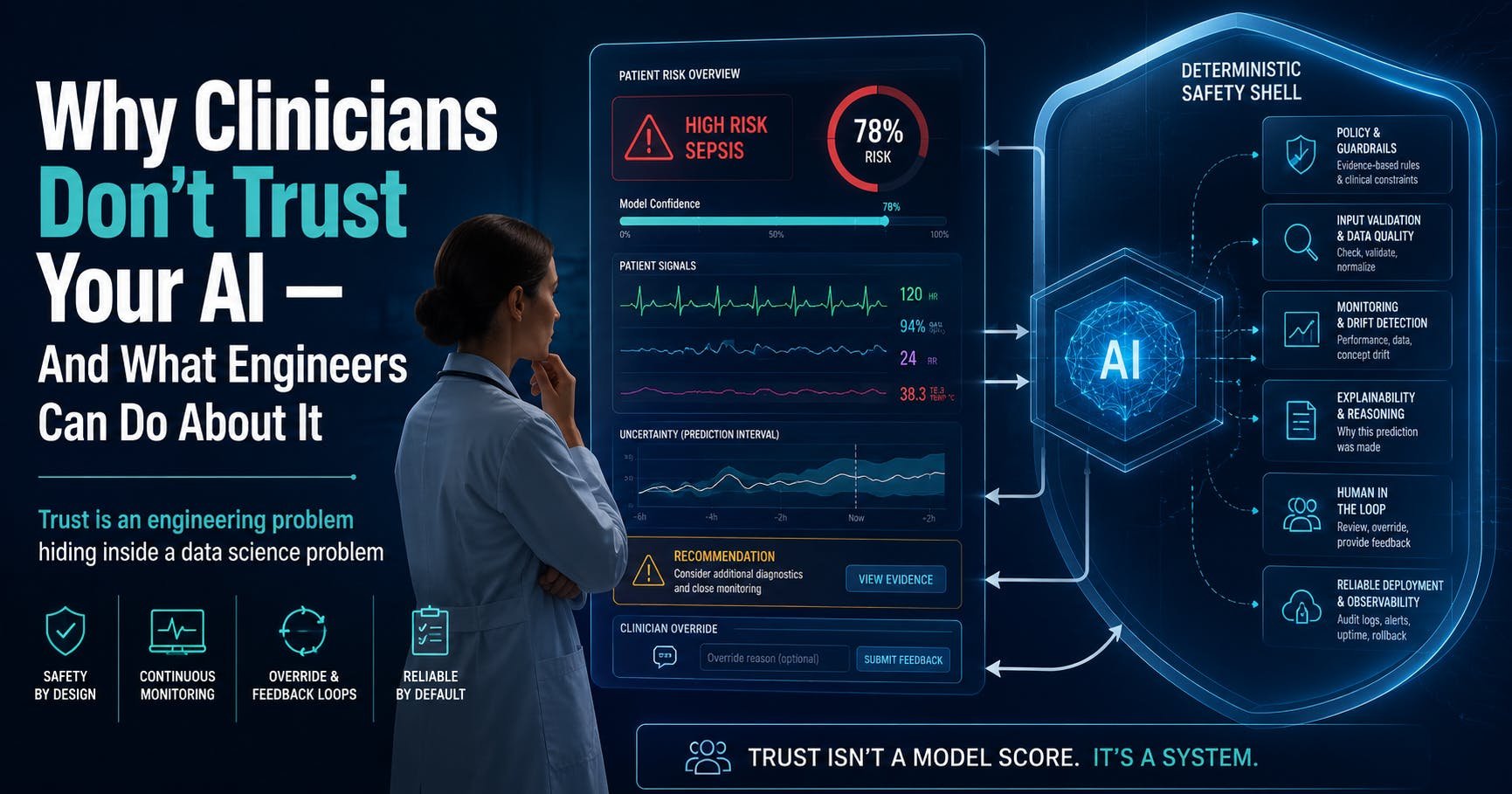
Why Clinicians Don't Trust Your AI – And What Engineers Can Do About It
By Sujay Puvvadi, May 15 2026
The problem in a nutshell
A large hospital signed a contract to use a sepsis prediction model that boasted an AUC of 0.94. After months of integration work and training sessions, the system went live. Within a year‑and‑a‑half the alerts were silenced. Why? The model generated an alarm for every patient with a fever and a mildly elevated lactate, flooding ICU nurses with 40‑50 alerts per shift. Clinicians learned to ignore the warnings, and the system was quietly turned off.
That story mirrors the experience of the Epic Sepsis Model, deployed across hundreds of U.S. hospitals. Independent validation showed it missed 67 % of actual sepsis cases while producing a constant stream of false positives. Epic is not a shady vendor; it is the dominant EMR platform. The failure was not a fluke—it reveals a deeper mismatch between how the ML community measures success and what clinicians need in practice.
We’ve been solving the wrong problem
Most research labs chase higher AUC, larger models, and cleaner training data. Those metrics are useful in a benchmark, but they do not address the day‑to‑day reality of a busy ward. In 2025, 65.8 % of adult patients reported low trust in AI‑driven healthcare tools, and clinicians are the primary gatekeepers of that trust.
Three rational concerns dominate their skepticism:
- Silent degradation – models keep outputting confident scores even when data drift makes them wrong.
- Constant alarms without explanation – high‑frequency alerts erode attention and create automation bias.
- Inability to answer “Why?” – black‑box predictions provide no actionable reasoning, making clinicians feel blindsided when a recommendation is wrong.
The solution is not a bigger model; it is a system that fails gracefully, surfaces uncertainty, and learns from human overrides.
Failure mode #1 – The silent killer you’re not monitoring
In traditional software, a crash throws an exception and alerts the engineer. ML models, however, often keep running with high confidence even when the underlying data distribution has shifted—a phenomenon known as concept drift.
Example: During a hospital’s transition from ICD‑9 to ICD‑10 coding, a sepsis model’s AUROC dropped from 0.73 to 0.53. The model continued to emit risk scores, but those scores no longer reflected reality. The monitoring dashboards still showed green because the feature distributions looked normal.
What engineers can do
- Treat drift detection as a safety feature. Continuously track both model performance metrics (e.g., calibration error) and raw feature distributions.
- Set quantitative drift thresholds. When a feature’s statistical distance (e.g., KL‑divergence) exceeds a preset limit, trigger an alert to the clinical governance committee rather than the data‑science team alone.
- Automate rollback. Deploy a fallback rule‑based model or a “no‑alert” mode until the drift is investigated.
Failure mode #2 – Reasoning drift in agentic workflows
Agentic AI (e.g., autonomous order‑entry bots) introduces a new risk: reasoning drift. Small deviations in early steps can compound, leading the agent to take nonsensical actions such as looping on the same order or prescribing an unrelated medication.
Research finding: In long‑horizon tasks, output divergence can exceed 20‑30 %, far beyond acceptable clinical error margins.
Engineering guardrails
- Narrow the agent’s action space. The Doctronic platform, for instance, limits its agents to approving a predefined list of 191 low‑risk medications and forbids any new therapy initiation.
- Implement a deterministic safety shell around the probabilistic core. The shell enforces clinical invariants (e.g., dosage limits, allergy checks) and can intervene in three ways:
- Fail‑Safe: Block the output entirely and alert a human for life‑threatening errors.
- Fail‑Degraded: Switch to a simpler rule‑based recommendation when model uncertainty exceeds a threshold.
- Fail‑Operational: Activate a redundant backup model if the primary model shows drift.
- Adopt the FAME framework (Framework for AI Monitoring and Enforcement) to codify these fallback strategies.
The UI problem – Presenting confidence as fact
Most clinical AI dashboards display a single number, e.g., “Sepsis Risk: 83 %.” That phrasing implies certainty, which clashes with a clinician’s habit of juggling multiple differential diagnoses. The result is epistemic dishonesty and a loss of trust.
Three UI patterns that help
- Conformal Prediction – Return a set of plausible outcomes with a guaranteed coverage rate, e.g., “Patient likely has pneumonia or heart failure (95 % confidence).”
- Visual uncertainty bands – Show a risk distribution bar rather than a point estimate, letting clinicians see the confidence interval at a glance.
- Friction by design – For low‑confidence predictions, require a click‑through, a free‑text justification, or a “I have reviewed the chart” checkbox. This small hurdle interrupts autopilot behavior and reduces automation bias.
Turning overrides into a learning signal
Every time a clinician rejects an AI recommendation, they generate a labeled training example. Most systems simply log the event and discard it. By capturing overrides in a structured format (e.g., the Maria platform), you can feed them back into prompt‑adjustment pipelines and periodic retraining.
Pattern:
- AI drafts a note or order.
- Clinician reviews, edits, or rejects it.
- The system records the original suggestion, the clinician’s modification, and the context.
- Periodically, these examples are used to fine‑tune the model, improving both accuracy and alignment.
What to measure in production – Beyond AUC
AUC is a useful research metric but tells little about real‑world trust. Shift your dashboards to the following indicators:
| Metric | What it tells you |
|---|---|
| Override Rate | Percentage of AI suggestions rejected. High rates (>70 %) signal mistrust; low rates (<15 %) after a trust‑building rollout indicate acceptance. |
| Faithfulness Score | Alignment between the model’s explanation and its actual decision path. Low scores reveal “plausible but false” explanations. |
| Expected Calibration Error (ECE) | Does a 70 % confidence actually correspond to 70 % accuracy? Poor calibration harms both safety and trust. |
| Net Benefit (Decision Curve Analysis) | Does using the model improve patient outcomes compared to treating everyone or no one? This directly answers the clinical value question. |
A roadmap to incremental trust
The COMPOSER sepsis model at UCSD provides a concrete case study:
- 100 % human review of AI outputs during the pilot.
- Random audits of 10 % of cases after initial validation.
- Statistical monitoring with automatic rollback triggers.
- Iterative rollout as override rates fell from >90 % to 1.7 %.
Key takeaways:
- Define clear error criteria before deployment.
- Automate rollback pathways.
- Keep the clinical governance committee in the loop throughout.
Remember: patients are also users
Patient trust matters. Emerging Patient Comprehension Scores measure how well patients understand AI‑augmented diagnoses. A target of >90 % ensures informed consent and supports the broader doctor‑patient‑AI triad.
Bottom line
Clinicians aren’t irrational; they’re reacting to systems that:
- Degrade silently,
- Flood them with alarms,
- Hide uncertainty, and
- Refuse to explain their reasoning.
Improving raw model metrics won’t fix that. Engineers need to:
- Wrap models in deterministic safety shells,
- Surface calibrated uncertainty,
- Build phased autonomy that earns trust before scaling,
- Capture every override as a training signal, and
- Track trust‑centric metrics instead of AUC.
When the system, not just the model, becomes trustworthy, clinicians can finally let AI be a partner rather than a nuisance.
About the author
Sujay Puvvadi is a Software Development Engineer II at Amazon, focusing on AI agents that improve healthcare access. Follow him on Twitter for more insights on responsible AI in medicine.
Comments
Please log in or register to join the discussion