
A detailed examination of recent epidemiological trends shows that colorectal cancer (CRC) is indeed more common in younger cohorts than it was for their parents, but the increase is part of a broader rise in many cancers across generations. The post explains how cohort analyses differ from age‑band plots, evaluates proposed lifestyle and environmental causes, and argues that the most urgent public‑health response is expanded screening rather than chasing a single culprit.
The Core Claim
Recent headlines often proclaim that colorectal cancer is rising in young people. The statement is technically correct: people who are 20‑40 years old today have a higher incidence of CRC than people of the same age in the 1990s. Yet the phrase masks two deeper realities. First, the increase is not limited to a narrow age window; it is observable across the entire lifespan of later birth cohorts. Second, CRC is not an isolated phenomenon – a suite of cancers, from uterine to thyroid, shows similar generational upward trends.
How the Data Are Mis‑read
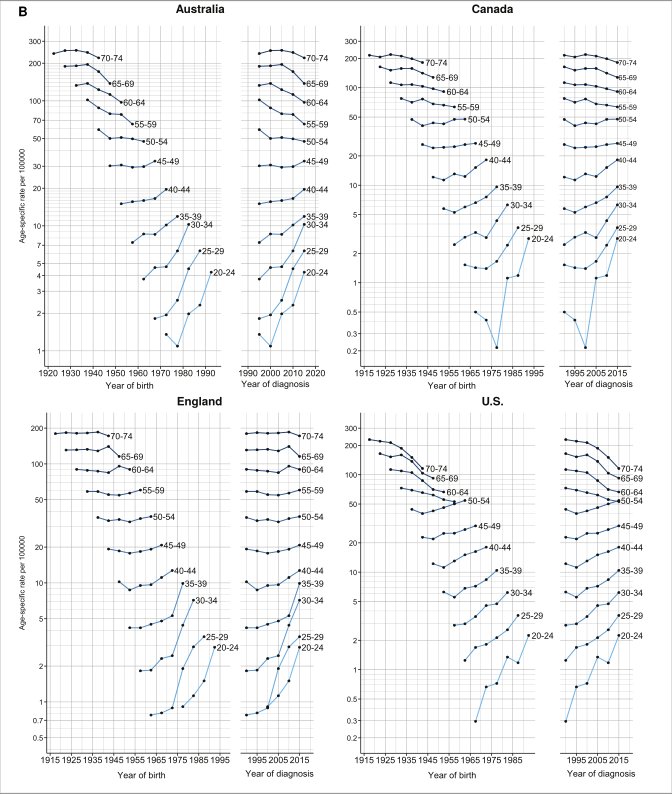
Epidemiologists traditionally present incidence by age band (e.g., 20‑24, 25‑29). When you compare a 2022 chart to one from 1995, the younger band appears higher, prompting the “young‑people” narrative. However, those bands contain different individuals at each time point. To understand whether a cohort – a group born in the same five‑year window – is experiencing a true shift, you must follow that cohort as it ages.
Cohort‑Based Plotting
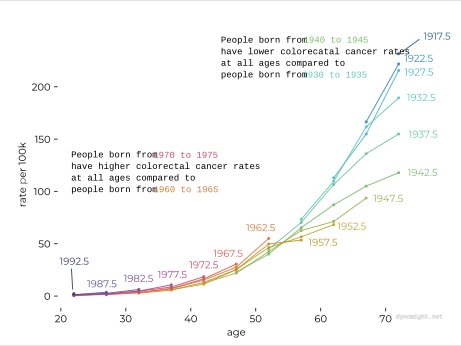
Siegel et al. (2026) and Downham et al. (2026) provide raw points for CRC incidence by age and year. By digitising those points and re‑plotting them so that each line represents a birth cohort (e.g., those born 1930‑1935), a clearer picture emerges:
- Cohorts born before 1950 enjoyed progressively lower CRC rates at every age compared with earlier generations.
- Starting with the 1950‑1960 birth window, the trend reverses: each subsequent cohort shows higher rates at all ages, from the twenties through the seventies.
This pattern suggests a generational exposure or set of exposures that affect the entire life course, not a factor that suddenly harms only the young.
Possible Drivers – A Reality Check
A dozen hypotheses have been floated, ranging from plausible to speculative. Below is a concise appraisal of each, focusing on the strength of epidemiological evidence and biological plausibility.
| Hypothesis | Evidence Strength | Comments |
|---|---|---|
| Obesity, physical inactivity, insulin resistance | Strong epidemiological association with CRC; rising prevalence in many countries. | These factors increase systemic inflammation and alter gut hormone signaling, which can promote tumorigenesis. However, they do not explain why the age‑specific rise is steeper than the overall rise in other cancers. |
| Ultra‑processed foods & low fiber | Moderate – cohort studies link high ultra‑processed intake to CRC, but causality is unclear. | Emulsifiers can disrupt the mucus barrier, allowing bacteria to contact epithelium, yet population‑level consumption trends are hard to quantify precisely. |
| Red/processed meat, nitrites, secondary bile acids | Consistent meta‑analyses show modest risk elevation. | The effect size is relatively small; dietary changes alone are unlikely to generate the observed generational jump. |
| Microbiome shifts (e.g., colibactin‑producing E. coli, F. nucleatum) | Biologically plausible; animal models demonstrate tumor promotion. | Human prevalence data are sparse, and there is no clear evidence that these strains have become more common over the past three decades. |
| Antibiotic exposure early in life | Some cohort data link early‑life antibiotics to later CRC, but confounding is substantial. | The trend in pediatric antibiotic prescribing has actually declined in many high‑income nations, weakening this as a primary driver. |
| Environmental pollutants (microplastics, PFAS, pesticides, air pollution) | Largely mechanistic speculation; human epidemiology is limited. | Exposure levels have risen, but the magnitude of risk for CRC remains unquantified. |
| Maternal metabolic health | Emerging evidence that maternal obesity can program offspring metabolism. | Long‑term follow‑up of offspring cohorts is still in its infancy; not yet a measurable population effect. |
| Screening bias | Weak – mortality from CRC is also increasing in younger cohorts, indicating that detection alone does not explain the trend. |
In sum, obesity‑related metabolic dysfunction and dietary patterns have the most robust data, but none singularly accounts for the steep generational climb. The most parsimonious interpretation is that multiple modest risk factors are acting together, producing a cumulative effect that becomes evident when you compare entire birth cohorts.
The Bigger Picture: Cancer Incidence Across Generations
Sung et al. (2019) compiled incidence trends for 20 cancer types worldwide. When plotted on a log‑scale, the upward trajectories for uterine, gallbladder, kidney, liver, pancreas, and thyroid cancers are strikingly similar to CRC’s. The logarithmic axis reveals that a quarter‑step between ticks corresponds to a ~1.8‑fold increase, underscoring that many cancers are becoming more common, not just CRC.
Why does CRC dominate public discourse? Three practical reasons:
- Prevalence – CRC remains one of the most common solid tumours worldwide.
- Treatability when detected early – Colonoscopy can remove precancerous polyps, turning a potentially lethal disease into a curable one.
- Screening feasibility – Non‑invasive stool‑based tests and colonoscopy are widely available, unlike effective screening for pancreatic or thyroid cancer.
Other cancers may be rising, but without a clear screening pathway, the public‑health impact of early detection is limited.
Implications for Public Health Policy
- Lower the age threshold for average‑risk screening – Many health agencies have already moved from 50 years to 45 years. The cohort data suggest that further reductions could capture a growing at‑risk population.
- Promote primary‑prevention strategies – While the exact causal mix is unresolved, policies that reduce obesity, improve diet quality, and limit ultra‑processed food consumption will likely blunt the upward trend across multiple cancers.
- Invest in cohort‑level data infrastructure – The difficulty of constructing true birth‑cohort incidence curves highlights a gap in public‑health surveillance. Linking cancer registries with longitudinal health records would allow researchers to track risk trajectories more accurately.
Counter‑Perspectives
Some experts argue that the perceived rise is an artifact of improved diagnostic coding and greater awareness among clinicians, especially for younger patients presenting with rectal bleeding. While coding changes can inflate incidence numbers, the parallel rise in mortality among younger cohorts weakens this argument; more deaths imply a genuine increase in disease burden, not merely better detection.
Another dissenting view emphasizes genetic predisposition – hereditary syndromes such as Lynch syndrome may be diagnosed earlier now, inflating incidence in the 20‑40 age group. Yet hereditary cases account for only ~5 % of all CRC, insufficient to drive the observed generational shift.
Concluding Thoughts
The headline “colorectal cancer is rising in young people” is both true and misleading. True, because later birth cohorts experience higher incidence at every age. Misleading, because the phenomenon is not confined to youth nor to CRC alone; it reflects a broader, multi‑cancer generational increase likely driven by a constellation of lifestyle, dietary, and environmental changes.
For individuals, the actionable message is clear: screen early and often. For societies, the challenge is to address the upstream drivers – obesity, poor diet, and environmental exposures – that are reshaping the cancer landscape for future generations.
References
- Siegel, R. L. et al. (2026). Age‑specific incidence of colorectal cancer in the United States, 1995‑2022.
- Downham, D. et al. (2026). Cohort trends in colorectal cancer across the Anglosphere.
- Sung, H. et al. (2019). Global cancer statistics 2018: GLOBOCAN estimates.
This article endorses colorectal cancer screening. While colonoscopy remains the gold standard, stool‑based DNA tests and flexible sigmoidoscopy are also effective options and should be discussed with a healthcare provider.
Comments
Please log in or register to join the discussion