MIT researchers built a gel-like oral formulation that coats the esophagus and pushes drugs like infliximab through one of the body's most impermeable tissue barriers. The interesting part isn't just the medicine. It's the screening rig they engineered to test which inactive ingredients actually loosen the cellular gates.
A team at MIT has developed an oral drug formulation that does something the esophagus normally refuses to allow: it lets large molecules pass through the tissue lining instead of sliding past it. The work, published today in Nature Biomedical Engineering, targets a clinical gap that has frustrated gastroenterologists for years. There are very few ways to treat disorders of the esophagus directly, so patients usually take systemic drugs that circulate through the whole body and carry side effects far beyond the area that actually needs treatment.
The senior author is Giovanni Traverso, an associate professor of mechanical engineering at MIT who also practices as a gastroenterologist at Brigham and Women's Hospital. That dual background matters here, because the core problem is less about pharmacology and more about transport physics. The lead author is Christina Karavasili, a former MIT postdoc now an assistant professor at Aristotle University of Thessaloniki.
Why the esophagus is such a hard target
The esophagus is built to move things along quickly. Anything you swallow passes through in seconds, which leaves almost no time for a drug to act locally. On top of that, the tissue is lined with stratified squamous epithelium, a dense, layered cell structure that is highly impermeable. It evolved to keep things out, and it does that job well.
That creates real clinical consequences. Eosinophilic esophagitis, an inflammatory condition driven by food allergies, can cause the esophagus to constrict to the point where swallowing food becomes impossible. Crohn's disease can inflame the esophagus too. The standard treatment for these conditions includes infliximab, an antibody that neutralizes tumor necrosis factor alpha (TNF-alpha), an inflammatory signaling protein. Infliximab works, but it is an immunosuppressant delivered systemically, which raises the risk of infection and other complications across the entire body to treat a problem confined to one organ.
The existing workarounds are limited. Injecting drugs directly into esophageal tissue is uncomfortable and has to happen in a clinic. One anti-inflammatory steroid is formulated as a thick mixture that lingers longer after swallowing, but it still struggles to cross that impermeable squamous layer. Lingering on the surface is only half the problem. Getting through the wall is the other half.
The engineering move: build a test rig first
The part of this work that should interest anyone who thinks in systems is how the team approached the search. Rather than guessing at formulations and testing them in animals, they built a screening apparatus that mechanically mimics the esophagus. The setup presses a sample of esophageal tissue between two vertical plates. A drug formulation gets poured in at the top, simulating the act of swallowing, and wells in one of the plates collect whatever makes it through the tissue.
This is a transport measurement device, and it turned the formulation problem into something quantifiable. Instead of asking whether a drug works, the team could ask exactly how much of it crossed the barrier under different conditions. That distinction is what makes the rest of the project tractable. You cannot optimize what you cannot measure, and there was no good way to measure esophageal absorption at the bench before this.
With the rig in place, the researchers screened roughly 100 different excipients, the inactive ingredients that shape how a drug behaves. They narrowed those down to a set of top candidates, then tested them in pairs. The most effective combination was two bile salts, sodium chenodeoxycholate and sodium cholate, working together. Pairwise screening matters here because the effect was combinatorial. The salts performed better in tandem than either did alone, which is exactly the kind of interaction a single-variable screen would miss.
How the formulation actually works
The mechanism splits into two jobs handled by two components. The bile salts handle transport. The team's data suggests they temporarily loosen the cell-to-cell junctions that normally seal the tissue, and they appear to do it by interacting with calcium ions that hold those junctions together. Pull away the calcium scaffolding and the gates between cells open up enough for larger molecules, including antibodies, to slip into the mucosal tissue.
"Our data suggest that the bile salts temporarily loosen these cell-cell junctions, mainly by interacting with calcium ions that help maintain junction integrity," Karavasili said. "This creates a more permissive pathway between the cells, allowing larger molecules to move into the mucosal tissue more efficiently."
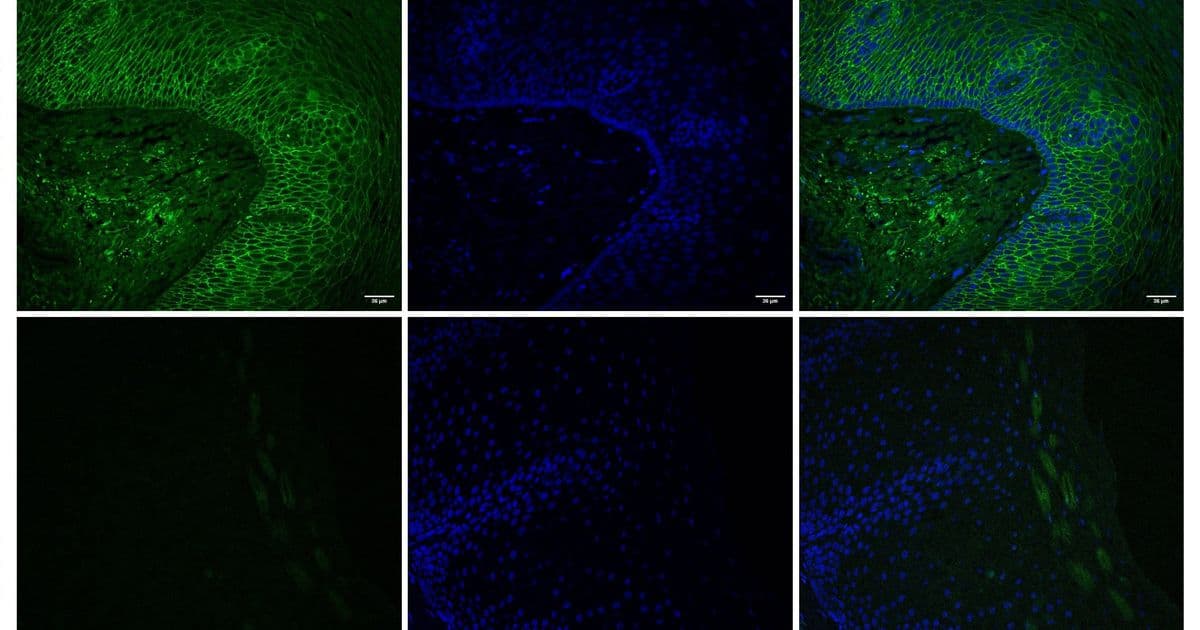
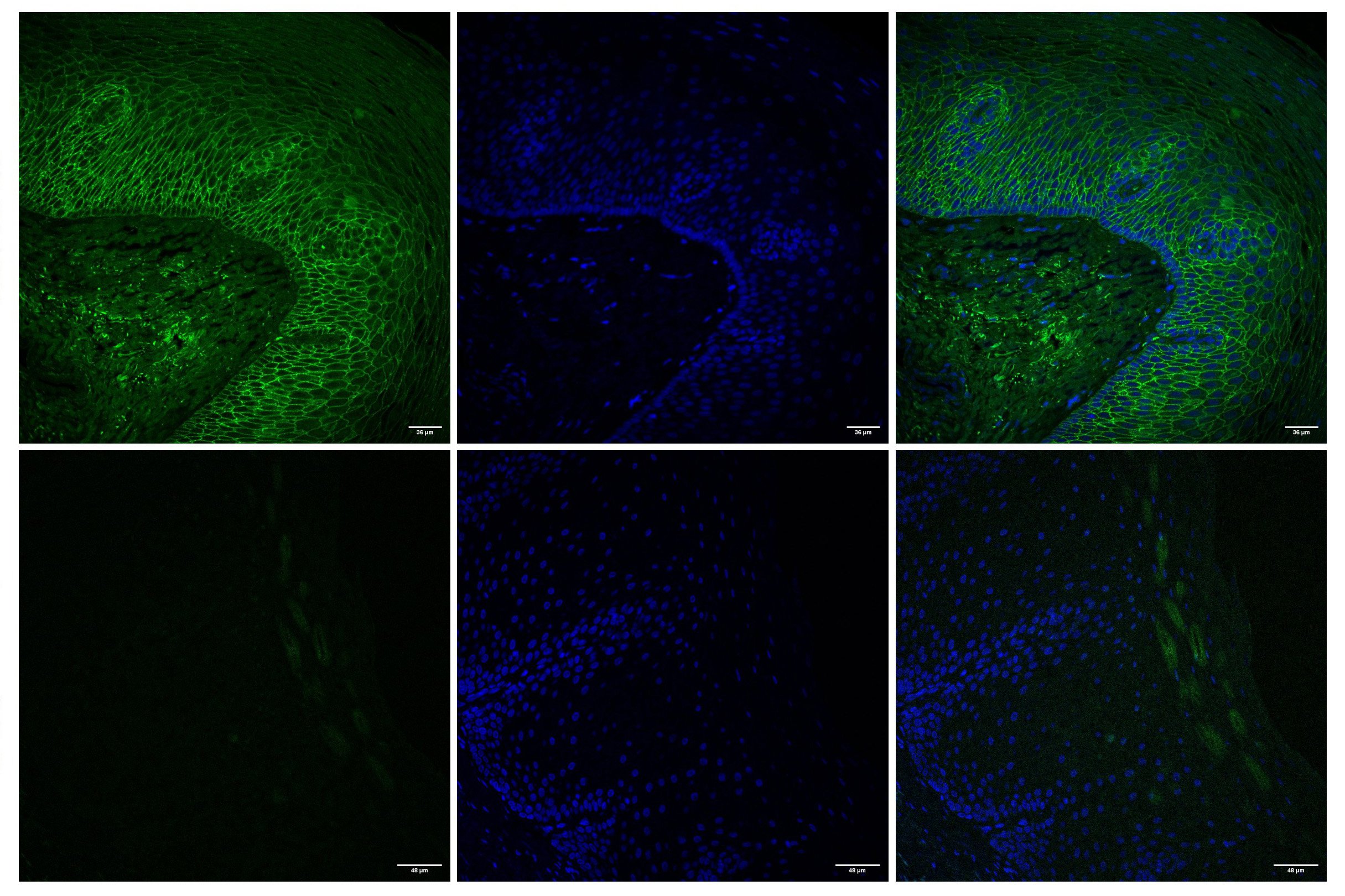
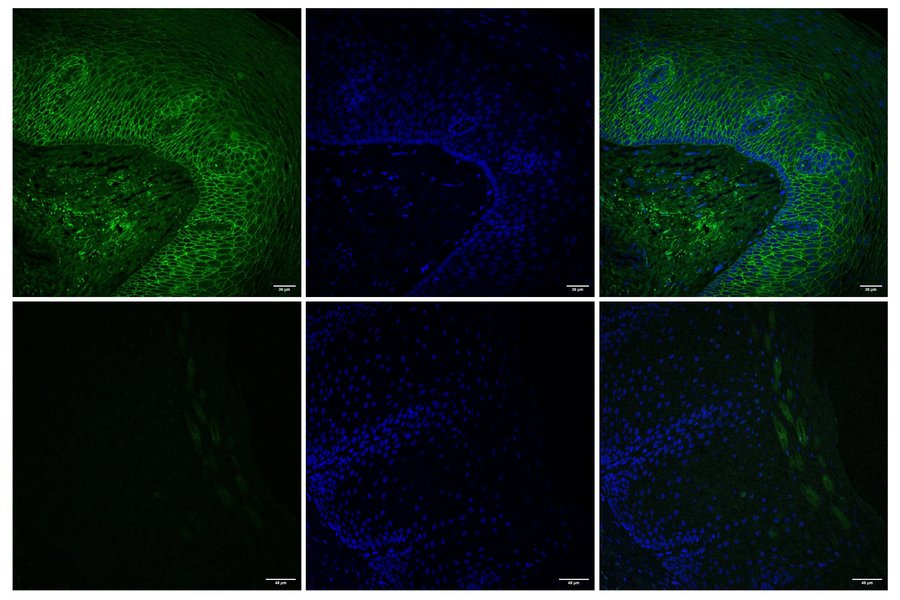
The second job is retention, handled by a polysaccharide-derived hydrogel. Its viscous consistency lets it lightly coat the esophageal lining so the formulation stays put long enough to do its work instead of being swept away in seconds. "The hydrogel helps the formulation remain on the esophageal surface for longer, while the bile salts help increase transport across the tissue," Karavasili said. The microscopy confirms the effect at the protein level. Imaging of E-cadherin, a protein that maintains connections between epithelial cells, showed a strong signal in untreated tissue and a reduced signal after treatment, consistent with that temporary loosening of the junctions.
The reversibility question
Anytime you deliberately compromise a biological barrier, the obvious worry is what happens after. A barrier that stays open is a liability, not a feature. The team tested this in animals and found that the loosening was temporary. The cells returned to normal within three days. That reversibility is what makes the approach plausible as a real therapy rather than a lab curiosity.
In those animal tests, the formulation delivered infliximab to the esophagus effectively. The clinical promise is straightforward: deliver the immunosuppressant where it is needed and spare the rest of the body the exposure. "If we have the possibility of site-directed delivery, we may be able to mitigate systemic side effects from these immunosuppressing agents," Traverso said.
What is still unsolved
The honest limitations sit mostly around timing and human translation. The team is now tuning how long the gel adheres. Too short and it cannot deliver the dose. Too long and it causes discomfort. That is a narrow window to hit, and animal results do not always carry cleanly into human anatomy and tolerance. The work has not yet been tested in people, and optimizing the formulation for human trials is the stated next step.
There is also the open question of how broadly this generalizes. The team framed infliximab as a model drug and is exploring whether the same platform can carry other antibodies and small-molecule drugs. Whether the bile-salt mechanism behaves the same way across different molecule sizes and chemistries remains to be shown.
Why this is a platform, not a product
The most useful framing comes from Traverso himself: "This is a platform to enable the development of drug-delivery systems for the esophagus, which hasn't been possible before because the tools haven't existed." The screening system is arguably the more durable contribution. A specific gel that delivers one antibody helps patients with one set of conditions. A reproducible way to measure and optimize esophageal drug transport lets other groups develop their own formulations without starting from zero.
This fits a broader pattern in Traverso's lab, which has produced ingestible devices for medication adherence, long-lasting drug delivery systems, and vibrating capsules aimed at obesity treatment. The common thread is treating the gastrointestinal tract as a mechanical engineering domain, where the constraints are about residence time, permeability, and physical placement as much as chemistry.

The research was funded by the Karl van Tassel Career Development Professorship, MIT's Department of Mechanical Engineering, the Division of Gastroenterology at Brigham and Women's Hospital, and ARPA-H. You can read more about the group's work at the Laboratory for Translational Engineering and through MIT's Department of Mechanical Engineering. The paper, titled "Oesophageal tissue screening system for assessing the retention and mucosal absorption of biologics," appears in Nature Biomedical Engineering.
For a field where the standard answer has been to flood the whole body with a drug and accept the collateral effects, a measurable, reversible way to deliver it to exactly one organ is a meaningful shift in what becomes possible.
Comments
Please log in or register to join the discussion